Mr Russell Hodgson

Copyright © 2017 Mr Russell Hodgson HPB and General Surgeon, Melbourne, Australia
Appointments/Enquiries: 9456 9511
Specialist HPB and General Surgeon
The pancreas is an organ with 2 major functions. It is mostly comprised of acinar cells that create enzymes and fluid to help digest food (exocrine function), and has small clusters of islet cells that produces a variety of hormones (endocrine function), the most common of which are the hormones that regulate sugar in our bloodstream: insulin and glucagon. The most common cancer of the pancreas arises from the acinar cells (adenocarcinoma) and is described here. Tumours that arise from the islet cells are called Neuroendocrine Tumours and are described here. Cystic tumours of the pancreas are rare forms of pancreatic cancer.
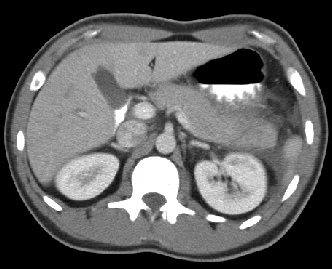
There are multiple types of cystic tumours of the pancreas including mucinous tumours (including Intraductal Papillary Mucinous Neoplasm (IPMN)), serous tumours and solid pseudopapillary tumours. Serous tumours are almost always non-cancerous and can often be left alone. The other forms of cystic tumours may require surgery.
IPMN is a pre-cancerous cystic lesion of the pancreas. There is a wide spectrum of IPMN with some very unlikely to ever cause malignant cancer, and others at high risk of progressing. Given the difficulty in treating pancreas cancer, it is important to treat those pre-cancerous lesions that are at high risk of progressing.
The monitoring and treatment of IPMN is one of the more debated areas of HPB surgery. In general the highest risk lesions often get treated with surgery. The other lesions may get further investigation or are simply monitored to ensure they do not change over time. Russell has experience in monitoring IPMN and deciding when and what type of surgery may be appropriate.